

















 Copy Link
Copy Link Share on X
Share on X Share on Facebook
Share on Facebook Share on LinkedIn
Share on LinkedIn
Always Active
Required for core functionality such as security, network management, and accessibility. These cannot be disabled.
Build intelligent AI systems that automate decisions, accelerate innovation, and scale business growth.
Design, build, modernize, and scale digital products that drive business growth.
Build secure, scalable, and intelligent platforms that power modern enterprises.
Build intelligent, connected, and autonomous systems that operate in the real world.
Flexible engineering capacity with predictable delivery, ownership, and outcomes.
Uncover the transformative potential of digital and mobile solutions for your industry

 Last Updated: Jul 15, 2026
May 26, 2026
Last Updated: Jul 15, 2026
May 26, 2026  439
439  29 min. Read
29 min. Read


Key Takeaways
Let’s evaluate your readiness and calculate your score in minutes
The most valuable data for healthcare AI systems (clinical histories, lab results, diagnostic imaging, treatment protocols) is also the most regulated. This creates what regulatory experts call the compliance paradox: the information that makes AI transformative in healthcare is the same information that, if mishandled, can trigger enforcement actions costing millions of dollars and years of corrective oversight.
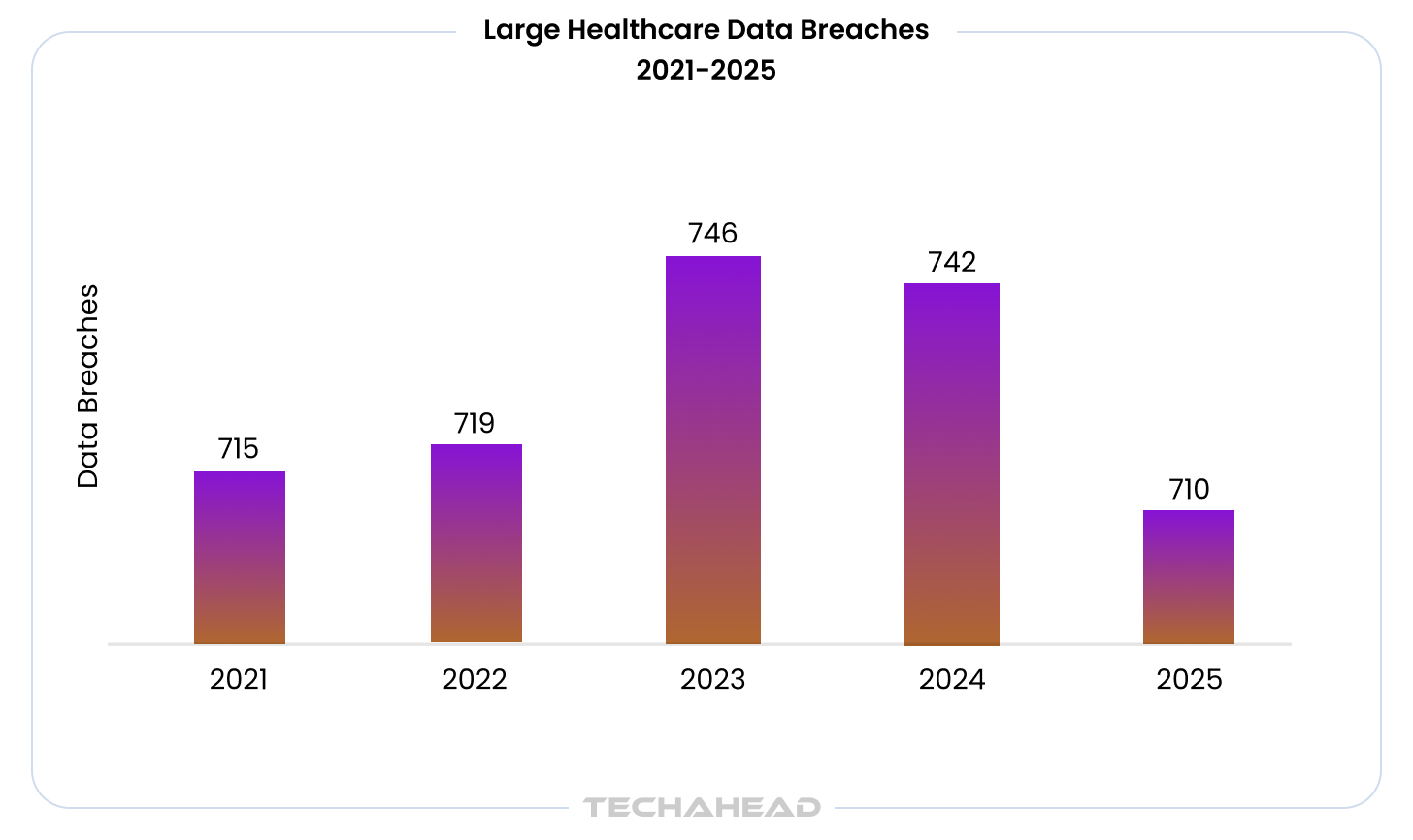
The stakes are rising as adoption accelerates:
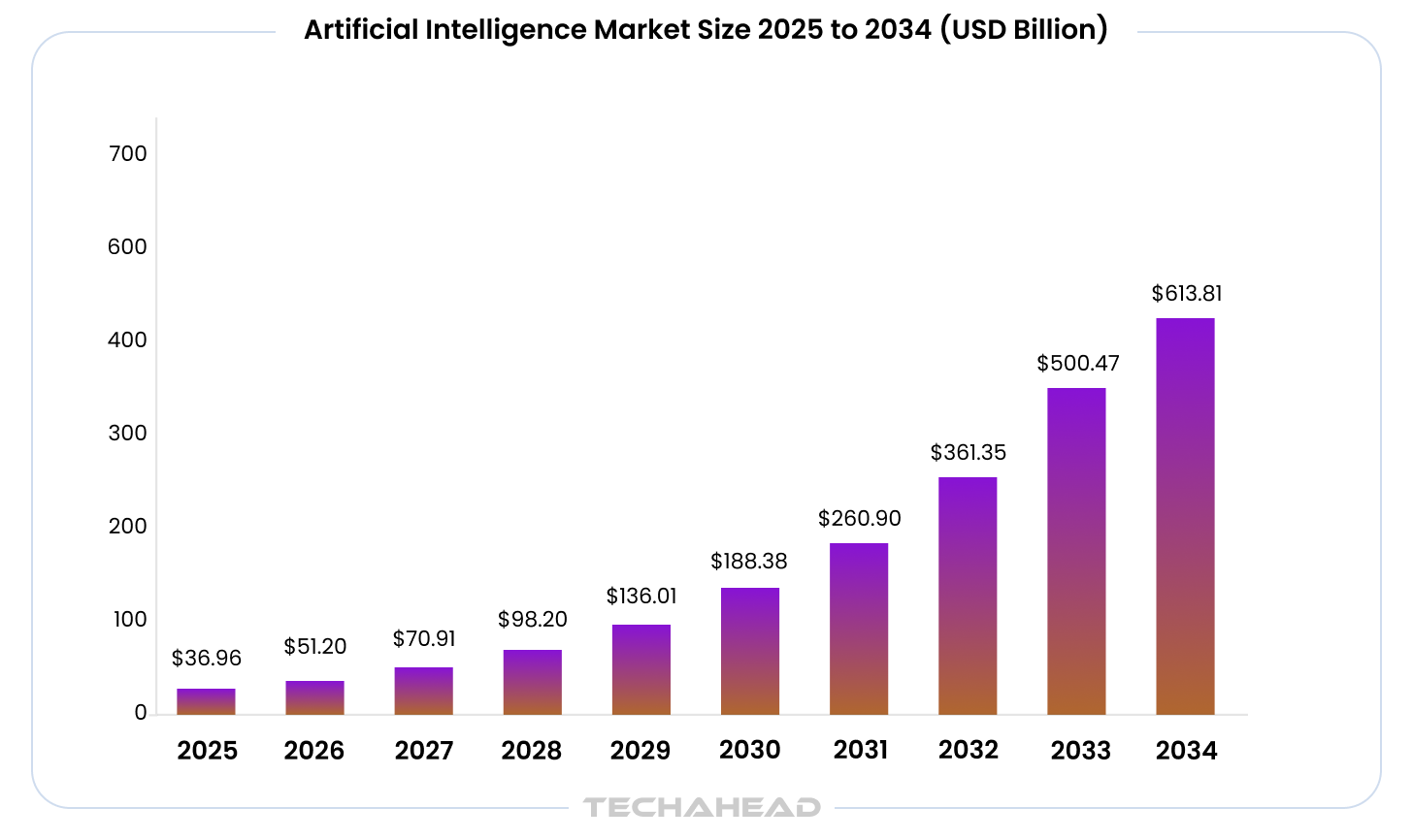
This isn’t experimental technology anymore. It’s becoming infrastructure. And infrastructure that handles protected health information needs compliant architecture from day one.
The challenge most organizations are facing: traditional software compliance strategies won’t protect you when AI processes PHI. When an AI model handles Protected Health Information through training pipelines, retrieval systems, and inference endpoints, PHI exposure occurs at layers that row-level database security was never designed to address. A chatbot summarizing patient records can inadvertently reproduce identifying details even when the underlying database access is perfectly controlled. A diagnostic assistant trained on clinical notes can embed PHI in model weights that persist long after the original data is deleted.
The organizations succeeding with HIPAA-compliant AI aren’t treating compliance as a post-development checklist. They’re designing it into system architecture from the initial technical specification, making PHI governance a foundational requirement that shapes data flow decisions, model selection, and infrastructure deployment before development begins.
This guide examines the architecture patterns, regulatory considerations, and development partnership criteria that determine whether your healthcare AI moves from proof-of-concept to production deployment without creating legal liability.
Recommended: Enterprise AI Compliance & Governance (2026)
An AI system is HIPAA compliant when it follows federal requirements under the Health Insurance Portability and Accountability Act to protect PHI and aligns with HIPAA standards. The HHS Office for Civil Rights resolved 21 HIPAA enforcement cases in 2025, with 76% including penalties for risk analysis failures, according to The HIPAA Journal Report.
More significantly, OCR (Office for Civil Rights) has expanded its enforcement focus from risk analysis to risk management, meaning you must now demonstrate not just that you identified compliance risks, but that you acted on them with documented remediation.
Compliance also requires meeting the core HIPAA rules: the Privacy Rule, Security Rule, and Breach Notification Rule.
Here’s what this means architecturally: A chatbot summarizing patient records can inadvertently reproduce identifying details even when the underlying database access is perfectly controlled. A diagnostic assistant trained on clinical notes can embed PHI in model weights that persist long after the original data is deleted. These aren’t hypothetical risks. They’re the attack surfaces OCR is actively investigating when violations occur. OCR enforcement matters because the average healthcare data breach now exceeds $10 million in cost, and the fallout can include penalties and lasting damage to patient trust.
Also Read: Navigating the Challenges of Connected Health in a Digital Age
Building AI systems that handle PHI requires architectural decisions at five critical layers. HIPAA applies to any AI system that creates, stores, or transmits protected health information, so healthcare teams must implement safeguards that protect patient data at every stage while maintaining the model performance that makes AI valuable in the first place.
In practice, HIPAA compliant AI tools are usually implemented through Business Associate Agreements, strict data minimization, and technical safeguards.
Bonus Read: How to Make Your Mobile App HIPAA Compliant?
Any third-party vendors handling PHI must meet the same privacy and security obligations under a BAA.
The foundational question in any HIPAA-compliant AI system is deceptively simple: where does patient data go when the AI processes it?
The answer determines your legal exposure, compliance requirements, and vendor relationships for the entire technology stack. Large language models from OpenAI, Anthropic, Google, and AWS can process PHI, but only under specific contractual and deployment configurations.
Here’s what you need to understand: The consumer versions of ChatGPT, Claude, and Gemini lack a business associate agreement. The enterprise API versions offered by AI vendors can be HIPAA-compliant when deployed through Azure OpenAI Service, AWS Bedrock, or Google Cloud’s Vertex AI, which provide the BAA coverage and infrastructure controls required for PHI handling AI systems.
A BAA should define permitted uses and disclosures of PHI, require subcontractors to meet the same obligations, and spell out each party’s security responsibilities.
Your LLM deployment options:
Some platforms also offer zero-retention processing to reduce retained customer data when configured appropriately.
The critical mistake organizations make: Using a consumer-tier LLM API and assuming it’s compliant because “we don’t send real patient names,” while also treating vendors that refuse to sign BAAs as acceptable when they should fail due diligence. HIPAA defines PHI broadly (any individually identifiable health information, including combinations of data that could identify a person). Sending “58-year-old female, diabetes, prescribed metformin, ZIP 90210” to a non-BAA provider is a violation even without a name.
TechAhead’s Approach to LLM Selection: At TechAhead, we evaluate LLM providers against three criteria before recommending deployment: BAA availability, FDA clinical decision support readiness (for diagnostic or treatment applications), and compatibility with ISO 13485 medical device software requirements. Our ISO 42001:2023 AI management system certification ensures these evaluations follow documented, auditable processes that regulatory bodies expect to see.
Recommended: Top AI Security Risks & How to Prevent Them
Traditional HIPAA compliance focused on database access controls. AI introduces three distinct attack surfaces where PHI can be exposed, and these must be secured under the HIPAA security rule.
When you fine-tune a model on clinical notes, PHI can become embedded in model weights. Large language models can reproduce verbatim text from training data under adversarial prompting. A model fine-tuned on an EHR corpus without rigorous de-identification becomes a latent PHI liability, regardless of access controls on the source tables.
Read more on the same on our Context Rot Blog
Understanding Safe Harbor de-identification: HIPAA’s Safe Harbor method requires removing 18 specific identifiers (names, dates, phone numbers, medical record numbers, and 14 others). If you miss even one identifier, or if re-identification is possible from the remaining data, it’s still PHI and fully covered by HIPAA requirements. This isn’t optional. De-identification for AI training must follow this standard or use the Expert Determination alternative method.
In RAG-based clinical AI HIPAA compliance implementations, the retrieval step surfaces PHI into the model’s context window. HIPAA‘s minimum necessary standard (45 CFR 164.502(b)) requires that PHI access be limited to what’s needed for a specific task. An AI agent scheduling a follow-up appointment might pull the full patient chart when all it needs is the patient’s name, provider, and preferred time slot. Row-level security doesn’t solve this. The agent retrieves far more than the task requires. Retrieval should happen inside a secure workspace to avoid exposing PHI beyond the immediate task context.
Least-privilege design with role based access controls helps ensure each user sees only the minimum data required for their function.
“We’ve seen healthcare organizations build RAG systems that pull 50KB of patient data when the AI task needs 2KB. The minimum necessary standard isn’t just a regulatory checkbox – it’s an architectural discipline. When we design retrieval systems for clinical AI, we treat every byte of PHI surfaced to the model as a compliance liability that must be justified.”
— Mukul Mayank, Chief Operating Officer, TechAhead
Recommended: Why Healthcare AI Need More Than RAG
Even when retrieval is controlled, LLMs can reproduce PHI in generated responses when those facts appear in the context window. A model summarizing highest-risk patients may surface individually identifiable information, even when the requesting coordinator is authorized only for de-identified population-level views. PHI should be secured with end to end encryption in transit and strong encryption at rest to protect PHI throughout processing and storage.
The vector database challenge: When patient data is embedded in vector databases for semantic retrieval, PHI is encoded as numerical representations. When a patient requests deletion under GDPR Article 17 or access under HIPAA, you must identify and act on every record, including those embedded in vector indices. Standard vector databases don’t support targeted deletion without complete provenance mapping of which source records contributed to which embeddings. Poor prompt or retrieval design can also cause data leakage.
Must Read: Agent Memory & State Management For Context-Aware AI Agents
If your AI provides clinical recommendations, you’re entering FDA territory. On January 6, 2026, the FDA published updated clinical decision support software guidance that directly affects how you architect healthcare AI systems.
The guidance clarifies that AI systems analyzing medical images to generate diagnostic recommendations remain subject to FDA oversight. Software providing a single clinically appropriate recommendation based on medical record text and clinical guidelines may fall outside FDA regulation if it meets all statutory criteria, but here’s the critical requirement: healthcare providers must be able to independently review the basis of the recommendation.
What this means for your architecture:
The FDA has cleared over 1,250 AI/ML-enabled medical devices as of May 2025. If your AI falls under device classification, you’ll need quality management systems compliant with 21 CFR Part 820. This is where ISO 13485 certification becomes relevant. It demonstrates your organization maintains the quality systems FDA expects for medical device software.
HIPAA requires audit trails not only for every PHI access, but also for edits, exports, and system actions involving PHI. For AI systems, this means logging more than most organizations realize:
Implementation requirements you can’t skip:
Breach-response workflows should let the vendor and healthcare provider quickly detect, contain, and mitigate unauthorized PHI exposure.
Bonus Read: Why Enterprise AI Need Audit Trails
OCR’s 2026 enforcement guidance makes clear: policies and written plans aren’t sufficient evidence of security measure implementation. They want to see actual logs, actual remediation actions, actual security controls in operation.
TechAhead’s Audit Trail Implementation: Our HIPAA-compliant AI architectures implement immutable audit trails using append-only log streams with cryptographic verification. Every PHI interaction is logged with full context lineage, from the original data source through retrieval, model inference, and final output. Our SOC 2 Type II certification validates these controls operate as designed, and our ISO 27001:2022 information security management ensures audit data itself is protected to the same standard as the PHI it documents.
Recommended: AI Development Guide 2026
When an AI hallucinates a drug interaction or fabricates a clinical guideline, the consequence isn’t a bad user experience. It’s a potential patient safety event. Your architecture must prevent hallucinations from reaching clinical decisions.
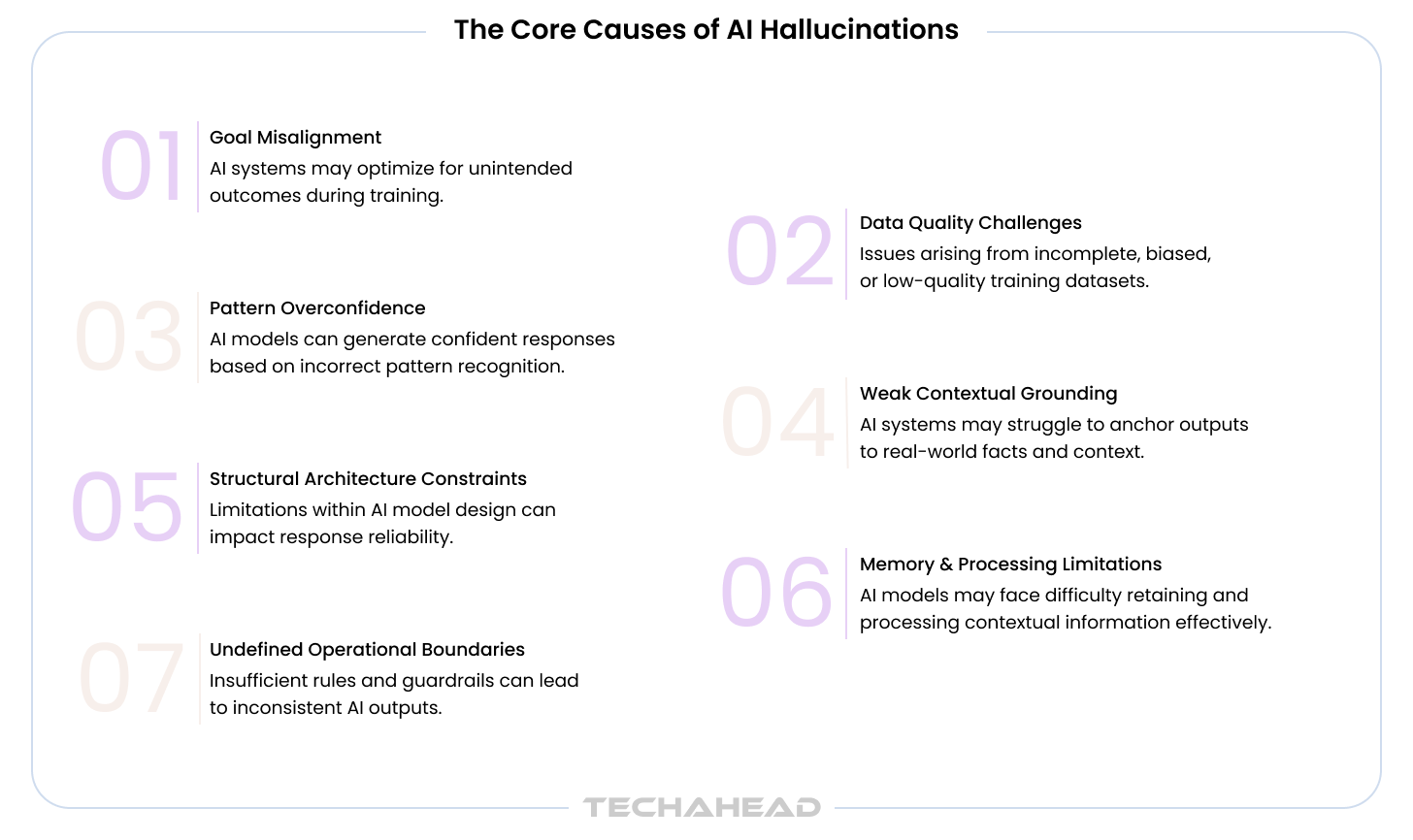
Three architectural approaches that work:
Retrieval-Augmented Generation (RAG) – The AI retrieves specific content from your verified knowledge base before generating a response, rather than relying on generalized model knowledge. This grounds responses in your actual policies and documentation.
Multi-stage validation – After retrieving content and generating a response, a separate validation step checks the response against source material. Claims that can’t be traced to a verified source are flagged or blocked.
Confidence-based escalation – The AI evaluates its confidence in each response. When confidence falls below threshold (often for complex or sensitive queries), the system escalates to a human agent rather than risking an inaccurate response.
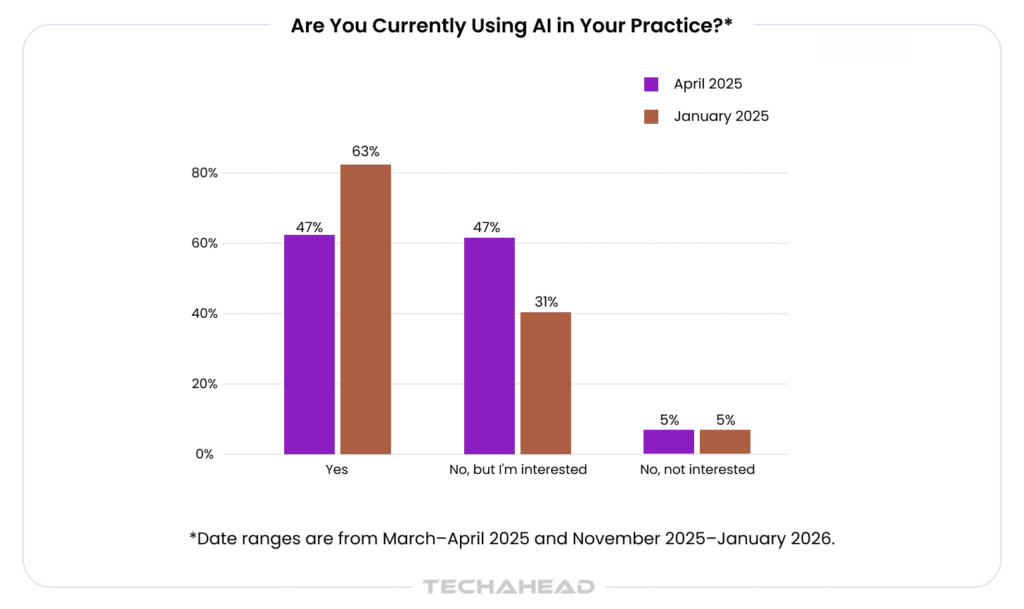
According to the Doximity 2026 State of AI in Medicine Report, 63% of US physicians now use AI tools, up from 47% just nine months earlier. But adoption doesn’t equal trust. Clinicians won’t act on AI recommendations they cannot trace. Explainability isn’t a nice-to-have feature. It’s the adoption barrier you must solve architecturally.
Related: Trends Toward Explainable Predictive Models
Before we discuss evaluating development partners, let’s examine the mistakes that derail most HIPAA-compliant healthcare AI projects. Recognizing these patterns helps you avoid expensive retrofitting and regulatory exposure.
If your architecture doesn’t account for PHI data flows from day one, retrofitting compliance costs 3-5x more than building it in. Compliance is an architectural decision, not a checklist you apply at the end. The Privacy Rule governs disclosures and patient rights, while the Security Rule requires safeguards that protect patient privacy. Organizations that treat HIPAA requirements as post-development tasks end up rebuilding core systems when OCR audits reveal fundamental data flow violations.
De-identification under HIPAA‘s Safe Harbor method requires removing 18 specific identifiers. If you miss one, or if re-identification is possible from remaining data, the data is still PHI and fully covered by HIPAA. Many organizations assume removing names and birth dates is sufficient. It’s not. Age above 89, five-digit ZIP codes, and 14 other identifiers must also be addressed.
ChatGPT (consumer), Claude (free tier), and Gemini (standard) do not have Business Associate Agreements. The models are the same as enterprise versions, but the compliance status is not. Using consumer APIs with PHI, even if “we don’t send names,” is a HIPAA violation. Enterprise deployments through Azure, AWS, or Google Cloud with signed BAAs are required. Compliance officers should train staff to distinguish approved organizational tools from unvetted generative AI.
Bonus Read: Guide to Developing Robust APIs
Embeddings generated from PHI are themselves PHI under HIPAA. They must be encrypted, access-controlled, and retained per HIPAA requirements. Most vector databases do not provide BAAs. Verify before storing PHI embeddings, and maintain complete provenance mapping for deletion requests.
An AI system that makes autonomous clinical recommendations without human oversight will not pass an OCR audit and creates patient safety liability. For FDA clinical decision support applications, human review isn’t optional. AI suggests, clinicians decide. This must be built into your workflow architecture. An AI assistant may support clinical documentation, patient instructions, or ambient intelligence only when it runs inside approved controls.
Not every AI development company can build HIPAA-compliant systems. The difference between vendors who’ve shipped production healthcare AI and those who’ve only built demos shows up in the questions they ask during scoping, the security documentation they provide during due diligence, and the certifications they hold before you sign a contract.
When you’re evaluating HIPAA AI development partners, these certifications demonstrate operational maturity:
SOC 2 Type II – Validates that security controls are in place and operating effectively over time (not just designed). This is the baseline for enterprise healthcare buyers. Type I is acceptable for startups; no certification is a red flag.
ISO 13485 – Medical device quality management system. If your AI falls under FDA device classification or handles clinical decision support, this certification shows your development partner understands regulatory requirements for medical software. Most AI development companies don’t hold this.
ISO 27001:2022 – Information security management. Demonstrates systematic approach to protecting sensitive data, including PHI.
ISO 42001:2023 – AI management system standard. This is cutting-edge, published in December 2023. Shows your partner has implemented governance specifically for AI system development, not just general software practices.
HIPAA attestation readiness – Can they sign a Business Associate Agreement before accessing any PHI? If they hesitate, they don’t have the infrastructure.
OpenAI Services Partner status – If they’re recommending OpenAI models, partner status indicates they’ve completed OpenAI’s technical and security reviews.
Must Read: Responsible & Ethical AI
Ask these during your technical evaluation. The answers reveal whether they’ve built production healthcare AI or just read about it:
| Question | Why It Matters | Red Flag Response |
| Will you sign a BAA before accessing any PHI? | Legal requirement | We’ll discuss that later |
| Do you have ISO 13485 certification? | Medical device software expertise | We have general ISO certs |
| How do you handle minimum necessary standard in RAG retrieval? | Shows architectural sophistication | Blank stares or ‘We retrieve everything’ |
| What’s your breach notification timeline? | HIPAA requires 60 days | Vague answer or ‘We’ll check’ |
| Can you provide a PHI data flow diagram for our specific use case? | Tests if they’ve done this before | Generic template response |
| Which LLM providers do you recommend and why? | Reveals if they understand BAA requirements | Recommends consumer ChatGPT |
“The difference between vendors who’ve shipped HIPAA-compliant AI and those still learning shows up in the first technical call. If they can’t sketch your PHI data flow architecture in 30 minutes, they haven’t done this before. Our clients don’t have budget for on-the-job training when OCR enforcement is rising.”
— Vikas Kaushik, CEO & Founder, TechAhead
Before you sign a development contract, these should be available for your review:
If they can’t produce these documents within a week of request, they probably don’t maintain them, which tells you about their operational maturity. Regular reviews of AI vendors against frameworks like the NIST AI Risk Management Framework should also be part of ongoing due diligence.
TechAhead’s Development Partner Positioning: As Claude & OpenAI Services Partner with ISO 42001:2023, and SOC 2 Type II certifications, TechAhead brings validated healthcare AI development processes to every engagement. We provide BAA execution, complete PHI data flow documentation, and third-party security assessments as standard deliverables, not premium add-ons, backed by production-grade HIPAA-compliant AI architecture for healthcare clients.
HIPAA-compliant AI costs more to build than non-regulated applications. Understanding where that cost comes from helps you budget accurately and avoid sticker shock when vendors present estimates.
Also Read: AI Chatbots Implementation Costs 2026
Here’s what production deployment actually takes when you do it correctly:
Total for production-ready MVP: 10-16 weeks minimum. Anyone promising faster delivery either has pre-built compliant infrastructure (ask to see it) or isn’t building compliance in from the start (which means costly retrofitting later). HIPAA requires regular security risk assessments to evaluate threats and impacts to PHI across AI workflows and infrastructure as part of ongoing compliance.
These ranges reflect what HIPAA-compliant AI actually costs when you include all required components:
| Project Scope | Investment Range | What’s Included |
| Proof of Concept | $50,000 – $100,000 | Single use case, limited PHI exposure, basic compliance architecture, cloud deployment with BAA |
| Production MVP | $100,000 – $200,000 | Full HIPAA compliance architecture, 2-3 clinical use cases, audit logging, SOC 2 preparation, FDA considerations if applicable |
| Enterprise Solution | $200,000 – $500,000 | Multi-system EHR integration, enterprise-scale deployment, full audit readiness, FDA submission support if needed |
The compliance tax: HIPAA compliance adds 30-50% to AI development costs versus non-regulated applications. This isn’t negotiable. It’s the cost of not paying $7.42 million average breach costs and avoiding multi-year corrective action plans from OCR.
Understanding these drivers helps you evaluate whether vendor estimates are realistic:
Infrastructure costs – BAA-covered cloud services (Azure, AWS, GCP) cost more than standard tiers, and some deployments may require a FedRAMP high environment for stricter security expectations. GPU infrastructure for self-hosted models runs $2,000-$10,000 monthly.
Security and compliance work – Penetration testing, security architecture reviews, compliance documentation, and audit log implementation require specialized expertise.
Integration complexity – Healthcare systems aren’t standardized. FHIR, HL7, proprietary EHR APIs – each integration point requires custom development and testing.
Regulatory considerations – FDA submission support, clinical validation studies, and device classification determinations add significant scope when your AI makes clinical recommendations.
HIPAA sets the federal floor for healthcare data protection, but state laws and international regulations can impose additional requirements that affect your AI architecture.
California Consumer Privacy Act (CCPA) health data provisions give California residents stronger rights around health information collected outside traditional HIPAA-covered entities. If your AI processes health data from consumer health apps, fitness trackers, or direct-to-consumer health services, CCPA’s health data protections apply even if HIPAA doesn’t.
Texas Health and Safety Code Section 181 (sometimes called “Texas HIPAA”) applies to covered entities in Texas and can impose stricter requirements than federal HIPAA for certain types of disclosures.
New York SHIELD Act requires reasonable safeguards for any private information, including health data, even for organizations not covered by HIPAA.
These state laws matter when you’re deploying AI that crosses traditional healthcare boundaries – employee wellness programs, consumer health apps, health data marketplaces. Your HIPAA AI development partner should ask about your deployment scope and flag applicable state requirements during architecture planning.
If your healthcare AI processes data of individuals in the European Economic Area, or if you operate clinical trials with EU participants, GDPR Article 9 protections for “special category” health data apply alongside HIPAA requirements.
Also Read: CCPA Vs. GDPR
Key GDPR requirements that affect architecture:
Data residency – PHI from EU patients must be processed within the EEA or in countries with adequacy decisions, unless you implement Standard Contractual Clauses. Your cloud provider choice (Azure EU, AWS Frankfurt, Google Belgium) becomes a compliance decision.
Right to erasure – EU patients can request deletion of their health data. Your vector database architecture must support complete deletion of embedded PHI, not just source records.
Consent management – GDPR requires explicit consent for processing health data in many contexts where HIPAA allows treatment/payment/operations. Your AI’s data usage must align with the consent you’ve obtained.
For US healthcare organizations with any EU data exposure (international patients, clinical trial participants, EU employee health records), both regulatory frameworks apply. Your architecture must satisfy the stricter requirement at each decision point.
Related: EU AI Act Compliance Checklist for Software Vendors
The healthcare organizations deploying AI successfully in 2026 share a common approach: they treat compliance architecture as a strategic enabler, not a regulatory burden.
When compliance is embedded in your initial technical architecture – when PHI data flow is mapped before model selection, when audit logging is designed before feature development, when FDA considerations shape your UX decisions – compliance becomes predictable, auditable, and defensible, especially when interfaces use plain language.
The alternative (building AI features first and addressing compliance later) leads to expensive retrofitting, delayed launches, and in the worst cases, systems that can’t be made compliant without fundamental rebuilds.
If you’re evaluating healthcare AI projects in 2026, start with architecture. The model you choose matters far less than whether your data flows, access controls, and audit trails can survive an OCR investigation.
The compliance paradox resolves architecturally. The richest and most restricted healthcare data are the same. Organizations that build the governance layer before the application layer cross from pilot to production.

Most HIPAA-compliant AI projects stall between proof-of-concept and production deployment because compliance wasn’t architected in from day one. TechAhead, as a healthcare development company builds healthcare AI applications where HIPAA requirements, FDA considerations, and audit trail architecture are embedded in the foundation itelf.
Since 2009, we’ve shipped 200+ HIPAA-compliant healthcare platforms (including 16+ industries) for Fortune 500 organizations and healthcare innovators. Our work spans Plunge’s IoT cold therapy platform (backed by Shark Tank’s Robert Herjavec), AXA’s AI-powered enterprise transformation, Unchecked Fitness’s AI platform delivering 85% user retention increases, JLL’s Intellicommand managing 5.4 billion square feet of property worldwide, and FitLine’s data-driven wellness ecosystem, among many others. Each project required production-grade HIPAA compliance architecture that passed real-world regulatory scrutiny.
What differentiates TechAhead in healthcare AI development:
Ready to build healthcare AI that ships to production without compliance delays? Connect with TechAhead to discuss your project requirements and receive a compliant architecture roadmap within two weeks.
No. Public AI tools like ChatGPT, Claude, or Gemini don’t offer Business Associate Agreements for standard accounts, meaning PHI processed through them creates HIPAA violations. You need enterprise versions with BAAs and zero-retention policies for HIPAA-compliant AI deployment.
Look beyond basic BAAs. Demand ISO 13485 for medical device software, ISO 42001:2023 for AI governance, SOC 2 Type II for security controls, and ISO 27001:2022. These prove your HIPAA AI development partner maintains FDA-grade quality systems and auditable processes.
Yes, absolutely. If your healthcare AI system creates embeddings from patient records, those vectors can be reverse-engineered to recover original data. Research shows 92% inversion success rates, making embeddings subject to HIPAA encryption and access control requirements.
HIPAA-ready means the vendor has infrastructure that could support compliance. HIPAA-compliant AI means they’ve signed a BAA, implemented all required safeguards (encryption, audit trails, access controls), and passed third-party security audits. Never confuse marketing language with actual compliance.
Yes, but only with proper safeguards. Your HIPAA-compliant AI architecture must use de-identified data, implement minimum necessary standards, maintain complete audit trails of PHI access, and ensure training happens in HIPAA-compliant environments with signed BAAs from all infrastructure providers.
Enterprise healthcare AI projects typically require 10-16 weeks. This includes architecture design (2-3 weeks), compliance infrastructure setup (3-4 weeks), development (4-6 weeks), security testing and HIPAA audits (2-3 weeks). Rushing compliance creates gaps that OCR investigations will expose.
Ask: “Will you sign a BAA before accessing PHI?”, “Where is our data stored when the contract ends?”, “Do you use our PHI to train your models?”, “What’s your breach notification timeline?”, and “Which third-party subprocessors touch our data?” Vague answers are red flags.
It depends. If your healthcare AI analyzes medical images for diagnostic recommendations or provides clinical decision support that clinicians rely on without independent review, you’re likely under FDA oversight. The 1,250+ cleared AI/ML devices show most clinical AI requires regulatory pathways.
Yes, if you process health data of EU residents. GDPR Article 9 treats health data as “special category” requiring explicit consent. Many US health systems now serve international patients or have EU research partnerships, making GDPR + HIPAA dual compliance standard practice.
This should be explicit in your BAA. Require certified data destruction within 30 days of contract termination, including backups, logs, and model weights trained on your data. Without contractual deletion timelines, your PHI handling AI systems create indefinite exposure windows after vendor relationships end.
Let’s evaluate your readiness and calculate your score in minutes
We use cookies to ensure our website functions properly, improve performance, and provide a personalized experience. You can choose which types of cookies to allow below.
Required for core functionality such as security, network management, and accessibility. These cannot be disabled.
Help us understand site traffic and user interactions so we can improve performance and usability.
Enable enhanced functionality and personalization such as language or region preferences.
Used to deliver relevant ads, track campaign performance, and measure advertising effectiveness.