Staff Augmentation
Access top-tier talent on demand: Dedicated, Hourly, or Flexible.

























 Copy Link
Copy Link Share on X
Share on X Share on Facebook
Share on Facebook Share on LinkedIn
Share on LinkedIn
Every year, at least 1 in 20 American adults experience a diagnostic error, according to 2024 data from ECRI, a global patient safety nonprofit. More critically, an estimated 795,000 Americans become permanently disabled or suffer from casualty annually from serious misdiagnosis-related harms, based on Johns Hopkins research published in BMJ Quality & Safety in 2024.
Key Takeaways
- AI clinical decision support delivers significant ROI within 14-16 months, with 50-55% diagnostic accuracy gains and up to 65% error reduction.
- Small pilots: $50K-$100K. Medium rollouts: $100K-$200K. Enterprise-wide: $200K-$500K+. Add 15-20% annually for maintenance.
- 15 diseases account for 50.7% of misdiagnosis harms (stroke, sepsis, cancer). Target these first for faster ROI and clinician buy-in.
- Model drift, integration failures, clinician resistance, data quality issues, and regulatory liability will derail deployments without systematic mitigation strategies.
- 96% of FDA-cleared AI uses the 510(k) pathway. HIPAA compliance costs $10K-$30K annually. Partner with SOC 2/HIPAA-certified vendors.
For healthcare systems navigating acute margins and mounting patient volumes, the stakes have never been higher. Artificial intelligence in healthcare is becoming the infrastructure that separates organizations that can scale quality care from those drowning in administrative overhead and preventable mistakes.
According to Nature, as of December 2024, the FDA had authorized over 1,000 AI-enabled medical devices for clinical use, with 96% cleared through the streamlined 510(k) pathway and radiology representing 76% of all approvals.
However, the real transformation isn’t happening in the algorithms themselves. It’s happening in how AI in clinical decision support changes the economics of diagnostic accuracy at enterprise scale. When a health system can reduce diagnostic errors while simultaneously cutting the time clinicians spend on documentation by 40%, you’re not just looking at better patient outcomes. You’re looking at a fundamentally different cost structure.
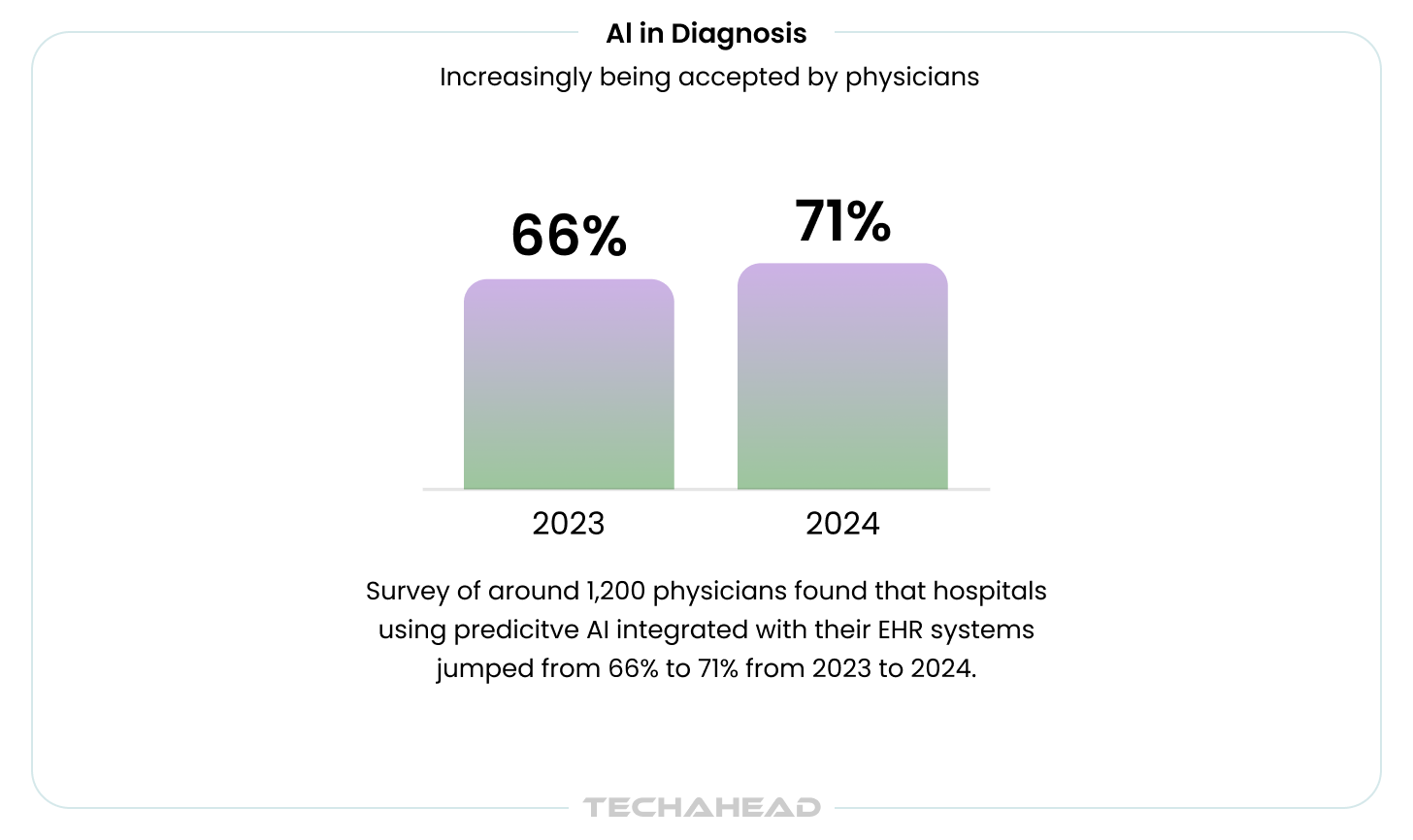
From 2023 to 2024, hospitals using predictive AI integrated with their EHRs jumped from 66% to 71%. The early movers aren’t waiting for perfect solutions. They’re betting that incremental improvements in accuracy, compounded across millions of patient encounters, creating competitive moats.

The Diagnostic Accuracy Gap Nobody Wants to Talk About
Let’s address a crucial aspect: Traditional diagnostic workflows, even in world-class health systems, carry an error rate that would be unacceptable in any other safety-critical industry. These aren’t edge cases or rare diseases.
We’re talking about conditions like:
- Sepsis, where timing is everything
- Stroke, where minutes determine outcomes
- Myocardial infarction, where delays cost lives
- Cancer, where early detection changes survival curves
This is where AI integration in healthcare is proving to be a game-changer.
The problem isn’t that clinicians lack competence. It’s that the diagnostic process itself is breaking under the weight of complexity.
Consider:
- A single patient encounter generates hundreds of data points across imaging, labs, vitals, medications, and history
- Medical knowledge doubles every 73 days
- The average physician has 8 minutes per patient
- Cognitive load increases while time per patient shrinks
This is where AI medical diagnosis starts making sense, not as a replacement for clinical judgment, but as a force multiplier for human cognition.
Also Read: Generative AI in Healthcare
How Machine Learning Actually Improves Diagnostic Outcomes
When AI in diagnostics systems work well, they don’t just match human performance. They exceed it in specific, measurable ways. Take breast cancer screening: AI-based diagnosis achieved 90% sensitivity compared to radiologists’ 78% in recent studies. That 12-percentage-point gap translates to lives saved.
And this isn’t limited to oncology. Across specialties, we’re seeing similar patterns where machine learning algorithms in healthcare like SVM (Support Vector Machine), HMM (Hidden Markov Model), Linear Regression, Logistic Regression, etc. deliver consistent accuracy that human practitioners struggle to maintain over long shifts.
Here’s what that looks like in practice. Modern AI diagnostic tools can:
- Process multimodal data (imaging, text, genomics) simultaneously, something human cognition struggles with
- Flag patterns invisible to the naked eye, detecting early-stage disease before clinical symptoms emerge
- Cross-reference patient data against millions of similar cases in real-time
- Maintain consistent performance regardless of fatigue, cognitive load, or time of day
- Provide second opinions at scale without adding headcount
Dr. Eric Topol, founder of Scripps Research Translational Institute, puts it plainly:
The machine will see things that humans will never see. It’s just extraordinary and this is why the hope for improving accuracy is so rich.
This insight captures exactly how AI improves diagnostic accuracy through pattern recognition that operates at scales beyond human perception.
Related Blog: Multimodal AI (Beyond Text and Images)
But let’s be clear. This isn’t about replacing radiologists or pathologists. The most effective implementations pair AI in clinical decision support with human expertise. It has been observed that when AI assists clinicians rather than working independently, diagnostic accuracy improves significantly compared to either approach alone.
The technology augments, not replaces. Smart health systems understand that the benefits of AI in clinical decision making compound when you treat it as a collaboration tool rather than a replacement strategy.
The Economics of Prevention vs. Treatment
Now here’s where things get interesting for the finance team. When you ask most development companies about the ROI of AI clinical decision support, they’ll talk about improved outcomes and patient satisfaction. All true, but the more difficult ROI question is:
“What’s the net present value of catching a disease six months earlier?
This is where partnering with a reputed healthcare development company who understands both technology and health economics becomes invaluable.
Consider the difference between early-stage and late-stage cancer treatment through AI medical diagnosis:
- Early detection: $50K treatment protocols
- Late-stage diagnosis: $200K+ treatment protocols
- Multiply across a population: fundamentally different economics
- Add reduced complications, shorter stays, better outcomes
You’re not just improving outcomes. You’re fundamentally changing the economics of care delivery. This financial impact is exactly why executive teams are increasingly prioritizing AI integration in healthcare over traditional IT investments.
Beyond cancer, the preventable adverse events story gets even more compelling. Diagnostic errors that lead to wrong treatments don’t just harm patients. They generate millions in additional costs.
The table below denotes hidden costs of diagnostics errors:
| Cost Category | Financial Impact |
| Extended hospital stays | Inappropriate initial treatment lengthens LOS |
| Complication management | Cascading treatment costs from wrong diagnosis |
| Malpractice insurance premiums | Higher premiums + claim settlements |
| Quality metric penalties | Lost revenue from CMS/payer penalties |
| Clinician turnover | Burnout and moral injury driving replacement costs |
According to a 2025 OECD health economics analysis report, halving diagnostic error rates could lead to savings of 8% of total healthcare expenditure. For a mid-sized health system with $1 billion in annual spending, that translates to $80 million in potential savings annually. When you factor downstream effects like reduced malpractice claims and improved patient outcomes, the ROI of AI clinical decision support becomes even more compelling.
Smart business executives like you model the complete financial picture. When evaluating implementation costs, they look beyond immediate expenses:
- Reduction in downstream treatment costs from earlier, more accurate diagnosis
- Decreased length of stay from appropriate initial treatment selection
- Lower malpractice insurance premiums and claim settlements
- Improved payer negotiations based on quality metrics
- Clinician retention through reduced burnout and documentation burden
The payback period? For most enterprise deployments of AI clinical decision support, break-even typically occurs within 18-24 months when you account for all these factors.
| Deployment Type | Break-Even Period | Notes |
| Enterprise AI clinical decision support | 18-24 months | When accounting for all financial factors |
| High-volume specialties (radiology, pathology) | Even faster returns | Volume amplifies ROI at scale |
Key Insight
Most organizations calculate ROI the old way – technology costs only. The real economic transformation happens at the system-wide level: early detection, reduced complications, lower malpractice exposure, and improved quality metrics.
What AI Implementation for Clinical Decision Support Actually Looks Like
Implementing artificial intelligence in healthcare at scale is less about the algorithm and more about change management, data infrastructure, and workflow integration. This is where the difference between a competent healthcare software development company and a subpar one becomes clear.
Start Narrow, Win Fast
The successful deployments we’ve seen don’t try to transform everything at once. They share a pragmatic approach:
Pick one high-volume, high-impact use case rather than trying to do everything at once. Radiology departments often lead because the workflow integration is cleaner and ROI metrics are straightforward. You can point to specific time savings per scan, accuracy improvements per case, and throughput gains per week.
Quick wins build momentum for larger initiatives. When your radiologists are discussing about how the AI caught something they missed, it’s much easier to get your cardiology department to pilot the next system. Success breeds adoption. Organizations pursuing healthcare digital transformation know that understanding how AI improves diagnostic accuracy doesn’t matter if clinicians won’t use it.
Workflow Integration That Actually Works
Most AI systems die not because the algorithm is bad, but because using them is annoying. The best systems integrate directly into existing workflows in ways that feel invisible:
- Appearing as natural extensions of the EHR rather than separate logins and interfaces
- Think seconds, not minutes, to get an AI recommendation
- Zero additional clicks wherever possible
- Seamless handoffs between systems
- Recommendations surfaced at the exact moment of decision-making
If your clinician has to open a separate application, log in again, copy patient data, wait for results, then manually transfer recommendations back into the chart, you are already behind the AI integration race.
Data Infrastructure: The Core Foundation
Third, they invest heavily in the data layer before touching any AI. Your technology partner should be asking hard questions about data quality, data interoperability standards, and cloud governance long before model selection. Garbage in, garbage out applies doubly when lives are on the line.
What this actually looks like:
- Auditing existing data completeness across your EHR (you’d be surprised how many required fields are blank)
- Establishing data validation rules at the point of entry
- Building ETL pipelines that can handle real-time feeds, not just nightly batch jobs
- Creating data governance committees that include both IT and clinical leadership
- Documenting data lineage so you know where every field comes from
This is where working with an experienced healthcare development company that understands FHIR, HL7, and clinical data models makes all the difference. If your technology partner can’t explain how they’ll handle your specific EHR’s quirks, that’s a red flag.
Must Read: AI-Driven EHR
Managing AI Implementation Risks (What Can Actually Go Wrong)
Let’s talk about the risks nobody mentions in the proof-of-concept phase. Deploying AI clinical decision support at enterprise scale introduces failure modes that don’t exist in traditional clinical IT. But the good news? Most are predictable and manageable if you plan for them upfront.
The table below summarizes the risks, impacts and mitigation strategies for each risk mentioned:
| Risk | Impact | Mitigation |
| Model Drift | Performance degrades 6-12 months after deployment as populations/protocols shift | Weekly dashboards, 5% drop alerts, quarterly retraining, 15-20% annual maintenance budget |
| Integration Failures | EHR/PACS upgrades break data pipelines; AI sits downstream of multiple systems | Sandbox testing, 30-day change notices, fallback protocols, documented runbooks |
| Clinician Resistance | <40% utilization = failed deployment; seasoned clinicians resist AI recommendations | Early clinical champions, frame as second opinion, celebrate catches without blame, opt-out initially |
| Data Quality | Missing labs, incomplete metadata, inconsistent coding degrade AI accuracy | Pre-contract audits, 95% completeness threshold, point-of-entry validation, separate remediation budget |
| Regulatory/Liability | Unclear legal accountability when AI suggests wrong treatment or misses diagnosis | Human-in-the-loop required, document all AI/clinician decisions, verify malpractice coverage, audit trails |
Model Drift: The Silent Performance Killer
This is the silent killer of AI diagnostic tools. Your AI model performs well in validation, then quietly degrades over 6-12 months as your patient population shifts, clinical protocols evolve, or new imaging equipment gets installed. A model trained on one demographic mix can perform poorly when your catchment area changes.
Mitigation strategy:
- Implement continuous monitoring dashboards tracking model performance metrics weekly
- Establish alert thresholds for sensitivity/specificity degradation (typically 5% drop triggers review)
- Contract for quarterly model retraining on your actual patient population
- Budget 15-20% of initial implementation cost annually for model maintenance
Your healthcare software development company should have automated monitoring infrastructure already built. If they’re offering annual check-ins instead of real-time dashboards, that’s a red flag.
Integration Failures and Data Pipeline Breaks
EHR upgrades, PACS system migrations, and vendor API changes will break your carefully orchestrated data flows. This is particularly painful with AI integration in healthcare because the AI system sits downstream of multiple source systems. One breaking change cascades into diagnostic recommendation failures.
Mitigation strategy:
- Demand sandbox environments for testing integration changes before production
- Establish change control processes requiring 30-day advance notice for any upstream system modifications
- Build fallback protocols so clinicians can continue working when AI systems are unavailable
- Maintain documented runbooks for common failure scenarios with expected resolution times
Clinician Resistance and Low Adoption Rates
You can build the most sophisticated AI for medical diagnosis platform in the world, but if utilization stays below 40%, you’ve failed. This isn’t a technology problem. It’s a change management problem. Radiologists who’ve practiced for 20 years don’t appreciate machines questioning their reads, even when the machine is right.
Mitigation strategy:
- Identify clinical champions early and involve them in vendor selection and pilot design
- Frame AI recommendations as second opinions, not replacements for clinical judgment
- Track and celebrate cases where AI caught what humans missed, without blame
- Provide opt-out mechanisms initially, then use data to demonstrate value before requiring adoption
- Invest in hands-on training, not just documentation and webinars
Data Quality and Completeness Issues
Your AI is only as good as the data it receives. Missing lab values, incomplete imaging metadata, inconsistent coding practices, and free-text notes instead of structured data all degrade its performance. Many organizations discover their data quality problems only after AI deployment begins.
Mitigation strategy:
- Conduct data quality audits before signing contracts, not after
- Establish minimum completeness thresholds (e.g., 95% of required fields populated)
- Implement data validation rules at the point of entry
- Build feedback loops showing clinicians when incomplete documentation impacts AI performance
- Budget for data remediation work as a separate workstream
Regulatory and Liability Exposure
Who’s liable when AI medical diagnosis suggests the wrong treatment path? What happens when a false negative leads to delayed cancer diagnosis? These questions don’t have settled legal answers yet, but you can’t wait for case law to develop before implementing safeguards.
Mitigation strategy:
- Maintain human-in-the-loop protocols where final clinical decisions rest with licensed practitioners
- Document AI recommendations alongside clinician decisions in the medical record
- Ensure malpractice insurance explicitly covers AI-assisted decision making
- Verify vendor’s liability insurance and indemnification terms
- Keep audit trails of all AI recommendations, overrides, and outcomes
The bottom line on risk management: Organizations that acknowledge these risks and plan for them systematically see benefits of AI in clinical decision making materialize faster than those pretending implementation will be smooth. Work with a healthcare development company that discusses failure modes openly, not just success stories.
Related: How to Align AI Capabilities with Business Outcomes
The Trust Problem (And How Leading Systems Are Solving It)
Dr. Karen DeSalvo, former Chief Health Officer at Google, nailed the core challenge:
“Health moves at the speed of trust.”
And right now, trust in AI systems is the rate-limiting step for adoption. This trust deficit affects every aspect of AI in diagnostics deployment, from initial physician buy-in to long-term utilization rates.
Why Clinicians Don’t Trust Black Boxes
Clinicians have legitimate concerns that go beyond typical technology skepticism. These aren’t theoretical objections. They’re the barriers preventing broader AI integration in healthcare across the industry.
The trust barriers:
- Black-box algorithms that can’t explain their reasoning? Hard pass
- Systems trained on homogeneous datasets that perform poorly on diverse populations? Dangerous
- Models that haven’t been validated in real-world clinical settings? Not dependable
- Vendors who can’t demonstrate performance metrics across patient demographics? Non-starters
When a radiologist can’t understand why the AI flagged a particular region on a scan, they’re forced to choose between trusting their own judgment or trusting an opaque system. Most choose their own judgment every time.
Building Trust Through Transparency
The organizations making progress are addressing trust through transparency and validation, not marketing promises. They’re doing the hard work that most vendors skip.
What transparency actually looks like:
- Publishing model performance metrics broken down by patient demographics
- Conducting prospective studies in their own patient populations, not just citing external research
- Building explainability features that show clinicians why the AI made a particular recommendation
- Creating feedback loops where clinician input improves model performance
Related: Top 10 Trends Towards Explainable Predictive Models
This commitment to transparency is what separates AI diagnostic tools that get used from those that gather dust. When clinicians can see the model’s reasoning, understand its limitations, and contribute to its improvement, adoption rates transform.
Human-in-the-Loop: The Adoption Accelerator
More importantly, they’re treating AI recommendations as exactly that: recommendations, not dictates. The final decision stays with the clinician, and the system tracks when clinicians override AI suggestions to continuously improve model performance. This human-in-the-loop approach maximizes the benefits of AI in clinical decision making while maintaining clinical autonomy.
The trust equation in practice:
Think of it like advanced GPS navigation. The system suggests a route, explains why it chose that route, shows you alternatives, and learns when you consistently choose a different path. You’re still driving. The AI is just a very smart copilot.
Must Read: Building AI Agents & Copilots that Integrate with Enterprise Workflows
Where AI Excels: The Disease Categories Seeing the Biggest Impact
Not all diagnostic errors are created equal. While AI in diagnostics can theoretically assist across the entire clinical spectrum, research shows the most dramatic improvements cluster around specific disease categories. According to a 2024 Johns Hopkins study, just 15 diseases account for 50.7% of all serious misdiagnosis-related harms, which makes them natural targets for AI clinical decision support deployment.
| Disease Category | Diagnostic Challenge | AI Performance Metrics | Clinical Impact |
| Stroke | Miss rates approach 40% for atypical presentations (dizziness, vertigo) | AI analyzes eye movement patterns + clinical presentation | Dramatic reduction in missed atypical stroke cases |
| Sepsis | Speed-critical; every hour delay increases mortality | AUC scores >0.88; FDA-authorized AI detection | Identifies at-risk patients hours before traditional protocols |
| Breast Cancer | High-volume screening requiring consistent accuracy | Improved detection rates across multiple clinical trials | Earlier detection; reduced false negatives |
| Lung Cancer | Early nodule detection in high-risk populations | Earlier nodule identification | Reduced late-stage diagnoses |
| Colorectal Cancer | Polyp detection during screening | Improved polyp detection rates with computer vision | Higher catch rates for precancerous lesions |
| Skin Cancer (Melanoma) | Visual pattern recognition under time pressure | Matches dermatologist accuracy in controlled studies | Consistent performance regardless of provider fatigue |
| Myocardial Infarction | Pattern recognition in emergency settings | Reduces diagnostic delays in ER | Faster time to intervention |
| Pulmonary Embolism | Subtle CT findings easily missed | Automated CT analysis catches subtle findings | Reduced missed diagnoses on imaging |
| Aortic Dissection | Overnight shift fatigue affects accuracy | Maintains diagnostic accuracy 24/7 | No performance degradation during overnight shifts |
Stroke leads the list, and the numbers tell a stark story. When patients present with classic symptoms like unilateral weakness, diagnostic accuracy is high even without AI. But when stroke manifests as dizziness or vertigo, miss rates approach 40% for isolated presentations. AI diagnostic tools analyzing eye movement patterns and clinical presentation are dropping these miss rates dramatically. That gap between “obvious” and “atypical” presentations is where AI saves lives.
Sepsis sits right behind stroke in terms of impact. The diagnostic challenge here isn’t complexity; it’s speed. Every hour of delay increases mortality risk. AI for medical diagnosis systems monitoring vitals, lab trends, and clinical notes in real-time are identifying at-risk patients hours before traditional recognition protocols catch them:
- Machine learning models predict sepsis onset with AUC scores consistently above 0.88
- Recent FDA authorization of AI-based sepsis detection demonstrates growing clinical validation
- Early warning systems flag deteriorating patients before obvious clinical manifestations appear
Cancer screening represents the volume play. The improvements compound across millions of screenings:
- Breast cancer: AI-assisted screening shows consistently improved detection rates across multiple clinical trials
- Lung cancer: Earlier nodule detection in high-risk populations reducing late-stage diagnoses
- Colorectal cancer: Polyp detection rates improving with computer vision assistance
- Skin cancer: Melanoma identification systems matching dermatologist accuracy in controlled studies
The cardiovascular event category shows similarly promising results:
- Myocardial infarction: Pattern recognition reducing diagnostic delays in emergency settings
- Pulmonary embolism: Automated CT analysis catching subtle findings
- Aortic dissection: Systems that don’t fatigue during overnight shifts maintaining diagnostic accuracy
Here’s what makes these specific disease categories particularly well-suited for AI integration in healthcare: they have clear diagnostic criteria, generate quantifiable data (imaging, labs, vitals), and carry severe consequences when missed. This is where understanding how AI improves diagnostic accuracy translates most directly into lives saved and costs avoided.
Organizations pursuing healthcare digital transformation see faster ROI and stronger clinician buy-in when they target these high-impact conditions first, then expand to broader applications once the value is proven.
Conclusion: Where This Is All Heading (And What to Do Now)
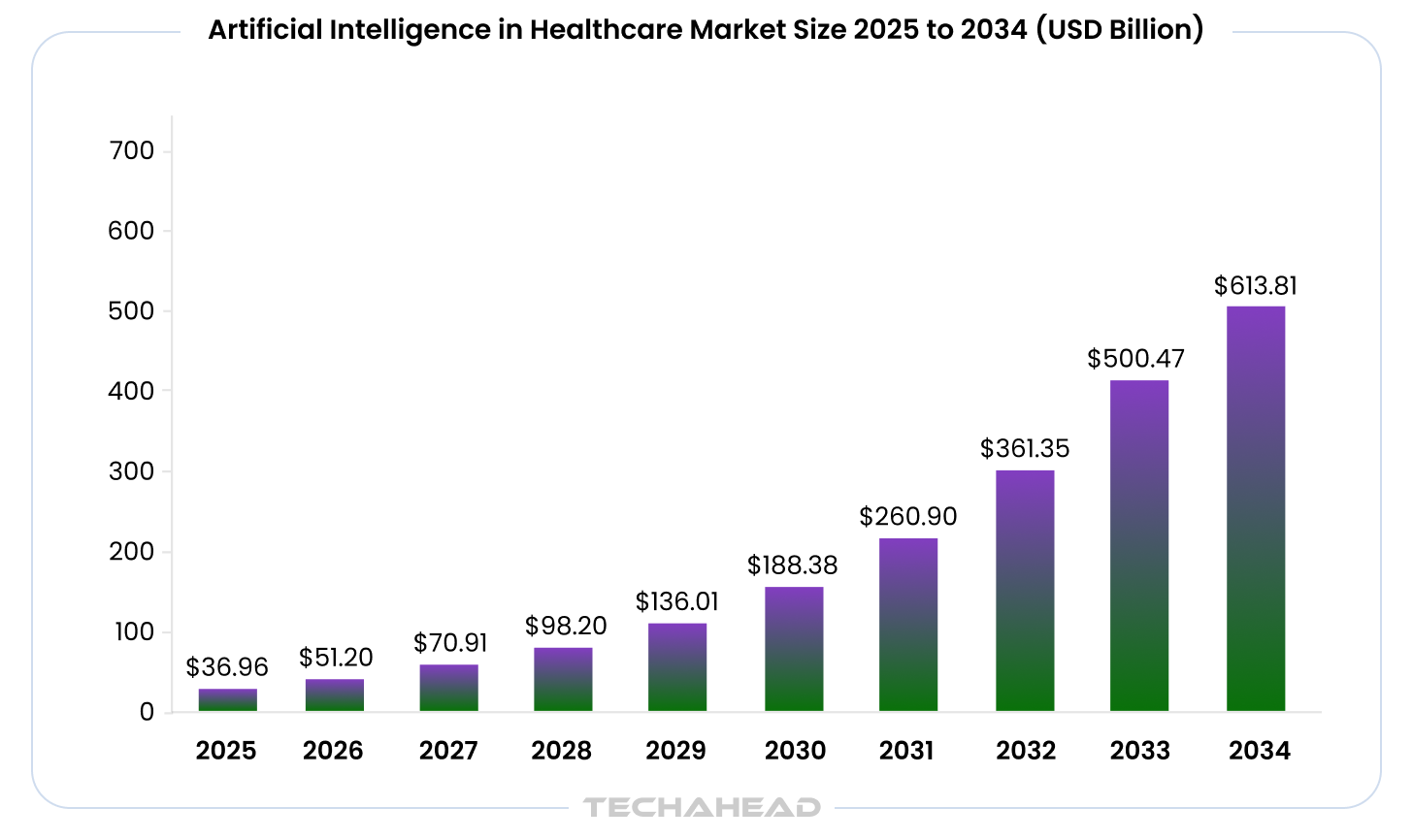
The trajectory is clear. By 2033, the global artificial intelligence in healthcare market is projected to exceed $500 billion. That’s not hype. That’s capital flowing toward solutions that demonstrably reduce costs and improve outcomes.
The healthcare digital transformation we’re witnessing isn’t a trend. It’s a fundamental restructuring of how care gets delivered.
What we’re seeing now, with AI in diagnostics focused primarily on imaging and radiology, is just the opening act. The next wave will bring:
- Multimodal systems integrating imaging, genomics, clinical notes, and real-time patient monitoring
- Ambient intelligence passively capturing patient-physician conversations
- Automatic EHR population with zero documentation burden
- Predictive models identifying patients at risk for diagnostic errors before they occur
- Pattern recognition invisible to traditional quality metrics
These advanced AI in clinical decision support systems will make today’s point solutions look primitive by comparison. This is the future of AI medical diagnosis that forward-thinking organizations are already piloting.
Organizations that partner with the right healthcare software development company today are building capabilities that will compound over years.
The organizations winning right now are those treating these initiatives as a strategic imperative rather than a nice-to-have innovation project. They’re:
- Building internal AI capabilities
- Partnering with proven technology companies
- Creating data infrastructure that can support increasingly sophisticated applications
Understanding that the ROI of AI clinical decision support extends far beyond immediate cost savings into strategic positioning for the next decade.
Start small if you need to. Pick one high-impact use case, prove the value, then expand. The need to start is now because the gap between early adopters and laggards is widening every quarter.
Why Choose TechAhead for Your AI-Powered Clinical Decision Support Deployment
TechAhead stands apart as a healthcare development company with 16+ years of proven expertise in deploying enterprise-grade AI solutions for Fortune 500 companies. Our track record includes partnerships with global leaders like Jones Lang LaSalle (JLL), American Express, Audi, and AXA, alongside specialized healthcare implementations for companies like The Healthy Mummy, Plunge, LearnENT, Jointhera, etc.
When it comes to AI-powered healthcare solutions, our credentials speak for themselves:
- SOC 2, GDPR, and HIPAA-compliant infrastructure built specifically for sensitive healthcare data
- Great Place to Work certified company with 240+ in-house specialists
- AWS Advanced Tier Services Partner with deep expertise in cloud-native AI deployments
- Recognized as Top Generative AI Company and Most Reviewed AI/ML provider (LA/India) by Clutch
We’ve delivered 2,500+ projects serving 1,200+ global brands, with our platforms supporting 500 million+ daily active users. Our approach combines Fortune 500 enterprise rigor with the agility needed to deploy clinical AI systems that meet strict regulatory requirements while delivering measurable ROI within months, not years.
Ready to reduce diagnostic errors and improve patient outcomes with AI-powered clinical decision support? Contact TechAhead today to discuss your implementation roadmap and see how we can transform your diagnostic accuracy at enterprise scale.
How much does it cost to implement AI clinical decision support in a hospital?
Implementation costs for AI clinical decision support depend on scope. Small deployments run $50K-$100K for single-department pilots. Medium projects? You’re looking at $100K-$200K for multi-specialty rollouts. Large implementations ($200K-$500K+) cover enterprise-wide systems. Add 15-20% annually for maintenance. The good news: most health systems hit ROI within 18-24 months.
How long does it take to implement AI-powered clinical decision support?
General AI integration in healthcare takes anywhere from 3-12 months, with enterprise deployments averaging around 17 months. But here’s what’s changed. Rapid-deployment firms now deliver production-ready systems in 2-4 weeks for focused use cases. You’re looking at discovery (1-2 weeks), prototyping (2-3 weeks), then optimization (6-12 weeks). After launch, expect continuous monitoring and model retraining every 3-6 months.
Is AI clinical decision support HIPAA compliant?
Yes, when implemented correctly. AI in diagnostics systems must meet full HIPAA requirements: data encryption, role-based access controls, audit logging, and Business Associate Agreements with vendors. Compliance setup runs $10K-$30K annually. You’ll need continuous monitoring, bias detection, and documentation of all AI recommendations. Work with SOC 2 and HIPAA certified development partners. That ensures regulatory adherence from day one.
Does AI clinical decision support require FDA approval?
It depends on what the system actually does. The FDA has cleared 1,000+ AI-enabled medical devices, 96% through the 510(k) pathway. Clinical decision support tools that support clinical judgment, not replace it, may be exempt under the 21st Century Cures Act. But AI making autonomous diagnostic recommendations? That typically requires 510(k) clearance, De Novo classification, or PMA approval. Partner with experienced healthcare development companies who understand FDA pathways.
What ROI can we expect from AI clinical decision support implementation?
Healthcare organizations typically see their ROI coming back within 14-16 months. Key drivers include 50-55% improvement in diagnostic accuracy, 30-40% clinician time savings, and up to 65% reduction in medical errors. Enterprise radiology deployments show 450-790% ROI over five years. Beyond financials, AI improves diagnostic accuracy through earlier disease detection. That translates to reduced downstream treatment costs and lower malpractice exposure.
How does AI clinical decision support integrate with our existing EHR system?
Modern AI clinical decision support integrates directly into EHR workflows using HL7 FHIR standards and APIs. It appears as a natural extension, not a separate application. Integration costs run $10K-$20K depending on EHR complexity. Best implementations surface AI recommendations at the exact moment of decision-making. Zero additional clicks. Your healthcare software development company should handle real-time data feeds, not just nightly batch jobs.
What experience should I look for in an AI clinical decision support vendor?
Look for proven artificial intelligence in healthcare deployments, not just polished demos. Key indicators: SOC 2, GDPR, and HIPAA compliance infrastructure already in place. Fortune 500 healthcare clients with verifiable case studies. AWS Advanced Tier or equivalent cloud partnerships. And at least 5+ years in healthcare AI development. TechAhead’s 16-year track record includes Fortune 500 partnerships and specialized healthcare implementations with measurable clinical outcomes.
How do we get clinicians to actually use AI clinical decision support?
Clinician adoption is the real challenge here. 61% cite workforce acceptance as critical. Start with high-volume, high-impact use cases that show quick wins. Frame AI in clinical decision support as a second opinion tool, not a replacement. Identify clinical champions early, provide hands-on training, and track cases where AI caught what humans missed. No blame. Human-in-the-loop approaches maintain clinical autonomy while building trust.
What data quality do we need for AI clinical decision support to work?
AI diagnostic tools require 95%+ completeness of structured EHR fields. Clean lab values, consistent imaging metadata, proper SNOMED CT/LOINC coding. Data preparation can cost $5K-$150K before AI development even begins. Conduct audits before vendor selection, not after. Establish validation rules at point of entry and document data lineage. Your technology partner should understand FHIR, HL7, and your specific EHR’s quirks. Upfront.
What ongoing maintenance does AI clinical decision support require after deployment?
AI in diagnostics requires continuous monitoring, not “set and forget.” Plan for model retraining every 3-6 months ($1K-$5K monthly), performance tracking dashboards with weekly metrics, and drift detection for accuracy degradation. When you see a 5% drop, that triggers review. Budget 15-20% of initial cost annually for maintenance. Partner with vendors offering automated monitoring infrastructure. Not just annual check-ins.